
Neonatal Jaundice
Aetiology
PHYSIOLOGIC JAUNDICE
o term infants: onset 2-3d of life, resolution by 2-3w
o premature infants: higher peak and longer duration
Pathophysiology
o increased hematocrit and decreased RBC lifespan
o immature glucuronyl transferase enzyme system (slow conjugation of bilirubin)
o increased enterohepatic circulation (refer to slideshow)
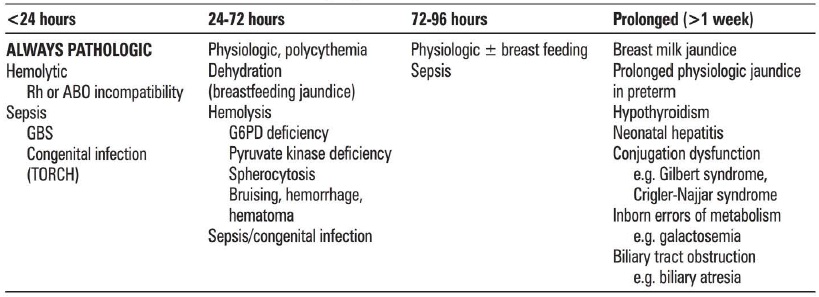
PATHOLOGICAL JAUNDICE
* Refer to above table
More importantly:
Too fast (<24 H)
Too long (>10 d)
Investigations
Management
Complications
Source
Toronto Notes 2012
www.rch.org.au 2014
- Exaggerated physiological response
o term infants: onset 2-3d of life, resolution by 2-3w
o premature infants: higher peak and longer duration
Pathophysiology
o increased hematocrit and decreased RBC lifespan
o immature glucuronyl transferase enzyme system (slow conjugation of bilirubin)
o increased enterohepatic circulation (refer to slideshow)
PATHOLOGICAL JAUNDICE
* Refer to above table
More importantly:
Too fast (<24 H)
- Haemolysis (ABO most common, Rh, G6PD)
Too long (>10 d)
- Biliary atresia ***must not miss this***
- Sepsis
- HypoTR
- Breast Milk Jaundice (dx of exclusion)
- rare (1 in 200 breast-fed infants)
- inhibitor of glucuronyl transferase found in breast milk
- onset 7 d of life, peak at 2nd to 3rd wk of life
- self-resolve 6-8 wk
- CONTINUE breastfeeding
Investigations
- Bedside: Urine dipstick (sepsis), urine MCS (SPA)
- Bloods: FBC/ CRP (sepsis), blood culture (sepsis), UEC (dehydration), SBR, blood typing (haemolytis), Coombs (haemolysis), maternal bloods, TFT
- Imaging: US (biliary atresia)
Management
- Correct dehydration (excretion via urine)
- Treat the cause
- Phototherapy (Special fluorescent blue light)
- TB monitoring 2-3h then 4-6 then 8-12 until N range
- Exchange transfusion (>25mg/dl)
- Kasai if biliary atresia
Complications
- Kernicterus
Source
Toronto Notes 2012
www.rch.org.au 2014
