
Asthma
Definition
Chronic airway obstruction caused by hypersensitivity that is reversible
Epidemiology
Children M>F 2:1, 15%
Adults M = F 10-12%
50% grow out of childhood asthma
Pathogenesis
Inflammation of airways --> hypertrophy of bronchiole epithelium/ sm + production of mucus --> airway obstruction
Aetiology
Clinical Features
Investigations
Management
NOTE: Avoid beta blockers (it causes bronchoconstriction)
Chronic airway obstruction caused by hypersensitivity that is reversible
Epidemiology
Children M>F 2:1, 15%
Adults M = F 10-12%
50% grow out of childhood asthma
Pathogenesis
Inflammation of airways --> hypertrophy of bronchiole epithelium/ sm + production of mucus --> airway obstruction
Aetiology
- Atopy
- Non specific trigger (exercise/ cold air)
Clinical Features
- Dyspnoea
- Productive cough
- Wheeze (may not be present)
- Pulsus paradoxus (SBP drop 10mmHg on inspiration)
- Reversible
Investigations
- Spirometry (FEV1 or FVC inc 15% = reversible) --> most common way of dx
- Exercise test, hypertonic saline, mannitol --> FEV1 dec = asthma
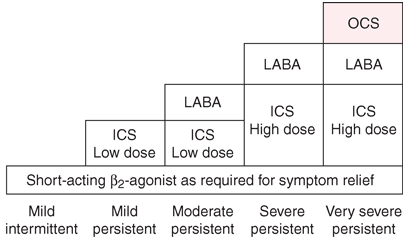
Management
- Education: Inhaler techniques (only 15% of pt have perfect techniques), asthma action plan (see below)
- In order of use:
- Sx reliever (relax peripheral SM, inhibit mast cells)
- SAB2A (2 puffs PRN) --> does not relieve sx as well
- LAB2A - salmeterol (Serevent/ Seretide), eformeterol (Symbicort)
- Preventer (suppresses inflammation)
- Inhaled corticosteroids - reduce exacerbation freq
- Oral CS
- Inhaled anticholinergics (prevent ACh bronchoconstriction/ mucus) = ineffective. Use if other inhalers aren't working.
- Leukotriene antagonist (montelukast) --> more useful in pt w salicylate sensitivity/ nasal polyps
- Theophylline (inhibit phosphodiesterase --> relax SM; rarely used)
- If inhaled steroids ineffective, use oral
NOTE: Avoid beta blockers (it causes bronchoconstriction)
Harrison's 18th Ed
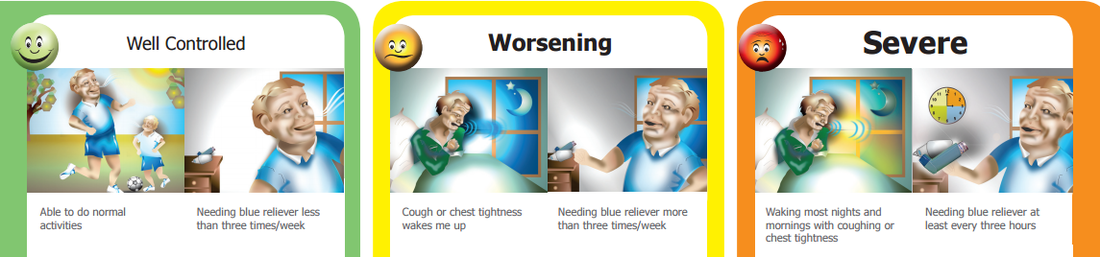
Asthma Action Plan (Asthma Foundation Australia 2015)
Acute severe asthma
O2 (aim SaO2 >90%) + inhaled SABA (nebuliser/ MDI)
+
IV SABA
+
Anti-cholinergic
+
Theophylline
+
MgSO4
+
Intubation
Details
MDI (puffer)/ spacer usage
Source
Dr Gregory Haug 2014
Toronto Notes 2012
O2 (aim SaO2 >90%) + inhaled SABA (nebuliser/ MDI)
+
IV SABA
+
Anti-cholinergic
+
Theophylline
+
MgSO4
+
Intubation
Details
MDI (puffer)/ spacer usage
Source
Dr Gregory Haug 2014
Toronto Notes 2012
