
Attention Deficit Hyperactivity Disorder (ADHD)
Epidemiology
DDX: learning disorders, hearing/visual defects, thyroid, atopic conditions, congenital
problems (fetal alcohol syndrome, Fragile X), lead poisoning, history of head injury, traumatic
life events (abuse)
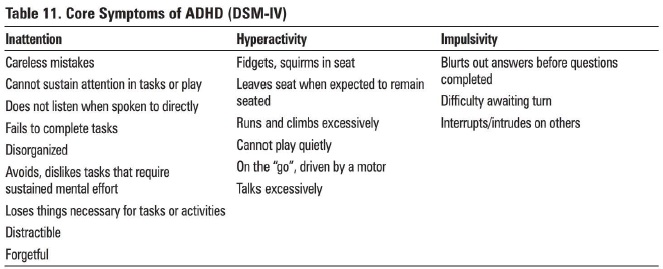
Diagnosis (3 subtypes):
Symptoms persist for >6 months
- Prevalence: 5-12% of school-aged children; M:F = 4:1, although girls may be under-diagnosed
- Girls tend to have inattentive/ distractible symptoms; boys have impulsive/hyperactive symptoms
- Genetic- dopamine candidate genes, catecholamine/neuroanatomical hypothesis
- Environment - Psychosocial, prem, toxins, diet, smoking/ alcohol during preg
- Cognitive - mental retardation, inhibitory control and other errors of executive function
- Arousal - alterations in the sensory system filters
DDX: learning disorders, hearing/visual defects, thyroid, atopic conditions, congenital
problems (fetal alcohol syndrome, Fragile X), lead poisoning, history of head injury, traumatic
life events (abuse)
Diagnosis (3 subtypes):
- Combined Type - 6 or more symptoms of inattention and 6 or more symptoms of hyperactivity-impulsivity
- Predominantly Inattentive Type - 6 or more symptoms of inattention
- Predominantly Hyperactive-Impulsive Type- 6 or more symptoms of hyperactivityimpulsivity
Symptoms persist for >6 months
- Onset before age 7
- Symptoms present in at least two settings (i.e. home, school, work)
- Interferes with academic, family, and social functioning
- Does not occur exclusively during the course of another psychiatric disorder
Features
Treatment
Prognosis
Source
Toronto Notes 2012
- average onset 3 yrs old
- identification upon school entry
- rule out developmental delay, genetic syndromes, encephalopathies or toxins (alcohol, lead)
- risk of substance abuse, particularly cannabis and cocaine, depression, anxiety, academic failure, poor social skills, risk of comorbid CD and/or ODD, risk of adult ASPD
- associated with family history of ADHD, difficult temperamental characteristics
Treatment
- non-pharmacological: parent management, anger control strategies, positive reinforcement, social skills training, individual/family therapy, resource room, tutors, classroom intervention, exercise routines, extracurricular activities
- pharmacological:
- standard treatment: stimulants (methylphenidate- Ritalin"', Concerta"' [long-acting]; Biphentin"'; dextroamphetamine; mixed amphetamine salts - Adderall"'; lisdexamfetamine (Vyvanse"'), SNRI (atomoxetine - Strattera"')
- for comorbid symptoms: antidepressants, antipsychotics
Prognosis
- 65% continue into adulthood; secondary personality disorders and compensatory anxiety disorders are identifiable
- 70-80% continue into adolescence, but hyperactive symptoms usually abate
Source
Toronto Notes 2012
