Developmental Dysplasia of Hip (DDH)
Risk Factors
5Fs:
F Hx
F emale
F irst Born
F rank Breech (buttock first with feet near head)
leFt hip
Aetiology
Clinical Features
Signs
5Fs:
F Hx
F emale
F irst Born
F rank Breech (buttock first with feet near head)
leFt hip
Aetiology
- Ligamentous laxity, muscular underdevelopment, and abnormal shallow slope of acetabular roof
Clinical Features
Signs
- Painless (if painful suspect septic dislocation)
- Diagnosis is clinical
- Limited abduction of the flexed hip ( <50-60°)
- Asymmetry in skin folds and gluteal muscles, wide perineum (due leg shortening)
- Barlow's test (for dislocatable hip)
- Flex hips and knees to 90° and grasp thigh
- Fully adduct hips, push posteriorly to try to dislocate hips
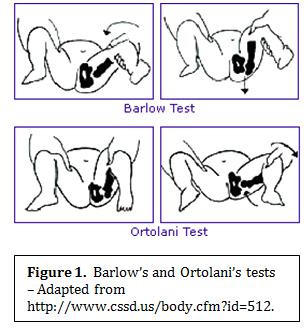
- Ortolani's test (for dislocated hip)
- Initial position as above but try to reduce hip with fingertips during abduction
- Positive test: palpable clunk is felt (not heard) if hip is reduced
Investigations
- U/S in first few months to view cartilage (bone is not calcified in newborns)
- Follow up radiograph after 3 months
Treatment
- 0-6 months: reduce hip using Pavlik harness to maintain abduction and flexion
- 6-18 months: reduction under GA, hip spica cast x 2-3 months (if Pavlik harness fails)
- > 18 months: open reduction; pelvic and/or femoral osteotomy
Complications
- Redislocation, inadequate reduction, stiffness
- AVN of femoral head
Source
Toronto Notes 2012
www.learnpediatrics.com
www.trulife.com
www.standfordchildrens.org

{kind=link}
{kind=link}