
Basic/ Advance Life Support (BLS/ ALS)
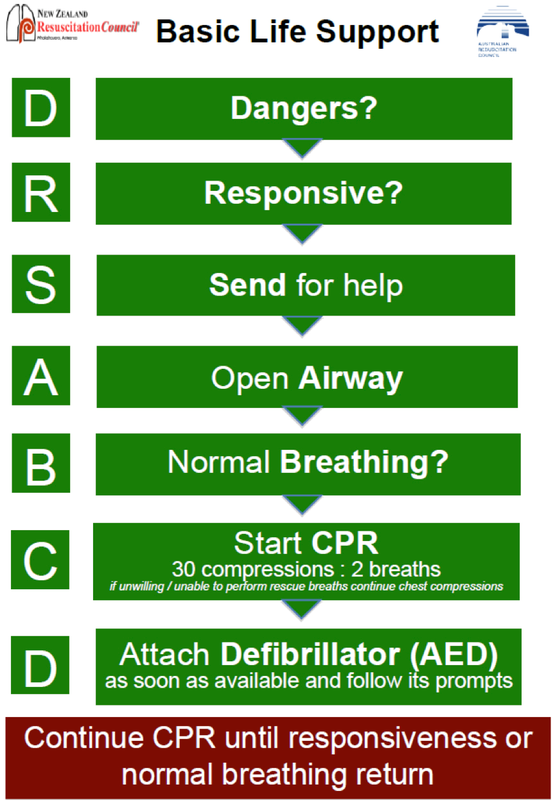
Dangers
Response
Send for help
Airway: Start compression if needed then fit airway adjuncts
If stridor present
1. Head tilt/ jaw thrust
2. Clear foreign body (if any), ill fitting dentures
3. Oropharyngeal tube (Guerdal)/ Nasopharyngeal tube/ Laryngeal mask/ Endotracheal tube
Guerdal (unsure)
Laryngeal mask (secure)
In secure airways (oesophagus), RR 8-12 BPM without stopping
If choking, sit them up
Breathing
Anaphylaxis
Circulation
Defibrillation
Manual
Response
- AVPU (alert, voice, pain, unresponsive)
- Sternal rub
- Supra-orbital pinch (nasally)
Send for help
- Emergency number/ MET call/ code blue
Airway: Start compression if needed then fit airway adjuncts
If stridor present
1. Head tilt/ jaw thrust
2. Clear foreign body (if any), ill fitting dentures
3. Oropharyngeal tube (Guerdal)/ Nasopharyngeal tube/ Laryngeal mask/ Endotracheal tube
Guerdal (unsure)
- Measure from tragus to corner of ipsilateral lip
- Watch out for loose teeth
- 1/3 into mouth --> rotate 180deg --> slide in (leave it free, not against lips)
- C/I with potential skull #
- Put into larger nostril --> push downwards (not backwards) with gentle twist
Laryngeal mask (secure)
- Can put in blind
- Seals oesophagus, prevent reflux aspiration
- Lube back, to avoid occlusion
In secure airways (oesophagus), RR 8-12 BPM without stopping
If choking, sit them up
- Leave them alone if coughing
- Otherwise, learn forward --> back blows with heel of hand, with another hand supporting sternum --> 3 x --> collapse --> chest compression
- Suction/ forceps
- Last resort: blow obstruction with mouth/ mask into R bronchus
Breathing
- Check trachea position
- Ear to mouth, eyes to chest
Anaphylaxis
- Adrenaline 0.3-0.5mg IM 1:1,000
- If hypovolaemic, unlikely to get rash due hypoperfusion
Circulation
- If cannot feel pulse, just do compressions (pt will react if circulation N)
- No radial pulse if SBP <80mmHg
- Compressions:
- 1/3 total chest diameter
- Allow for full recoil
- 100/min (to the beat of "Staying alive")
- Continuous compressions with secure airway (LMA/ETT)
Defibrillation
- If unsure about how to read rhythm, use AED/ auto mode
- If pads attached, but machine still say attach pad, check connection, pad seals
- Follow instructions
- Ensure everyone hands off before pressing shock
Manual
- Charge to 200J
- If non shockable, disarm then get back on chest
- Pulseless VT (wide, fat, fast)/ VF = shockable
- VT/VF causes: hypoxia/ meds/ drugs/ hypomagnesaemia/ congential defect --> acidosis --> electrolyte imbalance --> arrhythmia
- No pulse and electrical activity present = PEA
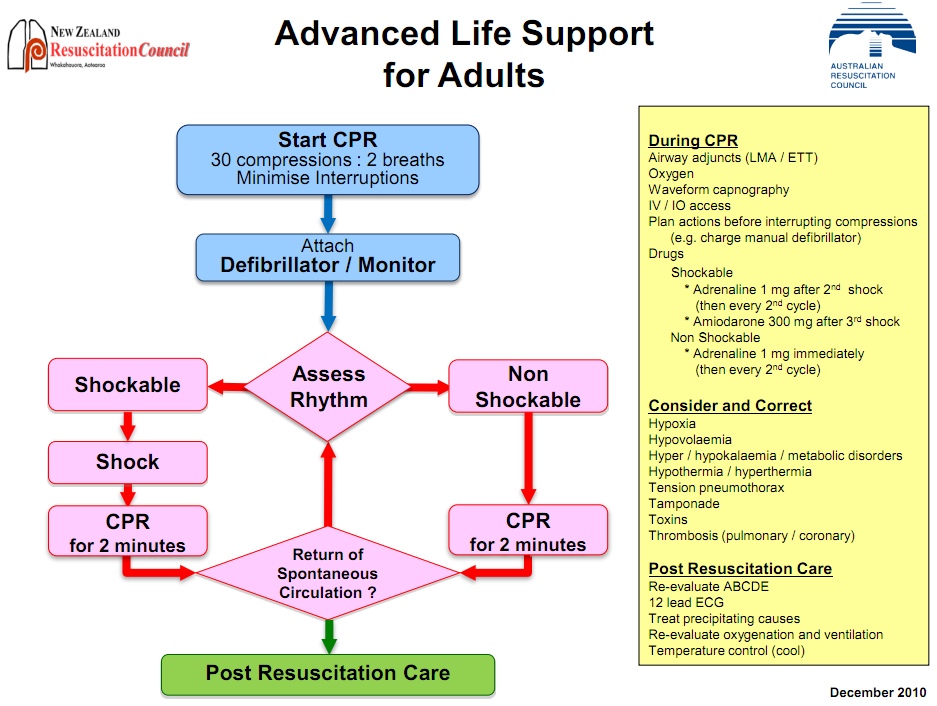
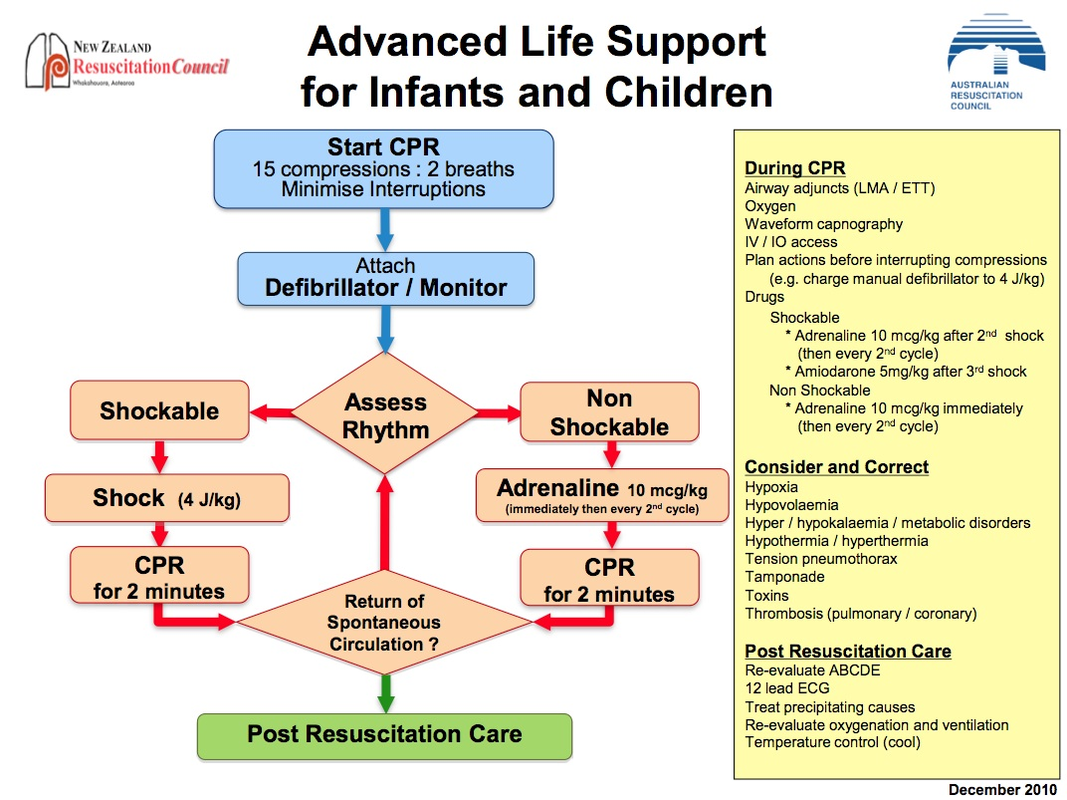
ALS (During CPR)
Airway adjuncts
Waveform capnography/ EZ cap
IV/IO access x 2
Drugs - Shockable
Drugs - Non-shockable
Causes (4H, 4T)
Hypoxia
Tamponade
Tension Pneumothorax
Thrombosis
Toxins
Return of Spontaneous Circulation
Source
Ms Vanessa Mee 2014
Australian Resusitation Council 2010
Airway adjuncts
- Secure airways preferred
Waveform capnography/ EZ cap
- Know CO2 levels
- ++ correct position + good ventilation (due expiratory CO2)
IV/IO access x 2
- 14-16G
- Fluids: 20ml/kg bolus
Drugs - Shockable
- After every 2nd shock: IV 1mg adrenaline 1:10,000 (usually give 1:1000 1mg/ml + 9ml N saline, then flush 20ml saline)
- After 3rd shock: IV amiodarone 300mg (give slowly, then flush with saline).
Drugs - Non-shockable
- 1:10,000 adrenaline immediately, then every 2nd shock (to get into shockable rhythm)
Causes (4H, 4T)
Hypoxia
- Most common cause of cardiac arrest in children
- Hypoxia --> Acidosis --> Electrolyte imbalance --> Cardiac arrest
- Commonly in elderly who fell
- Crush syndrome --> ++ K --> cardiac arrest
- Renal failure/ diarrhoea+vomiting
- Caused by: Blood loss, sepsis, spinal shock
Tamponade
- Caused by: pericarditis, post MI, Trauma
Tension Pneumothorax
- Caused by: Trauma, IPPV, asthma
- Sign: Initial HTN, then decompsate into hypotension
- Late sign: Tracheal deviation
Thrombosis
- Cardiac (AMI), Cerebram (CVA), Pulmonary (PE)
Toxins
- Common in children and elderly
- BB/ antidepressants/ suicide/ carbon monoxide (Rx: 100% O2)
Return of Spontaneous Circulation
- 2o surveillance
- Ensure >1 peripheral pulse
- Maintain BP
- Maintain temperature
- Treat cause
Source
Ms Vanessa Mee 2014
Australian Resusitation Council 2010
