
Stroke
SUMMARY
Clinical Features
Total ant circulation: hemiparesis/sensory, hemianopia, cortical signs
Partial ant circulation: 2/3 of above
Lacunar infarct: Any/ mixture of above without cortical signs
Post circulation syndrome: Brainstem/cerebellar features
--END OF SUMMARY--
Clinical Features
Total ant circulation: hemiparesis/sensory, hemianopia, cortical signs
Partial ant circulation: 2/3 of above
Lacunar infarct: Any/ mixture of above without cortical signs
Post circulation syndrome: Brainstem/cerebellar features
--END OF SUMMARY--
Definition
Stroke: Neurological deficits of vascular basis with infarct
TIA: without infarct, sx last <24h
Aetiology
Ischaemic (80%)
Haemorrhagic (20%)
Risk Factors
Stroke: Neurological deficits of vascular basis with infarct
TIA: without infarct, sx last <24h
Aetiology
Ischaemic (80%)
- Large vessel atherothrombosis/ emboli (most common: int carotid a)
- Lacunar (small vessel): htn cause vessel wall thickening (commonly: basal ganglia, int capsule, thalamus)
- Cardioembolic: AF, valvular disease, endocarditis, MI
- Systemic hypoperfusion: shock, HF
- Cerebral venous sinus thrombosis (Only sx = headache. rule out!!)
Haemorrhagic (20%)
- Intracerebral (ICH): htn --> aneurysm rupture (Charcot-Bouchard aneurysm) --> most common: putamen, thalamus, cerebellum, pons/ trauma/ vasculitis. drug use
- SAH
- Usually headache and hypertensive
Risk Factors
- HTN (most important)
- Smoking
- T2DM
Wikipedia
|
Wikipedia
|
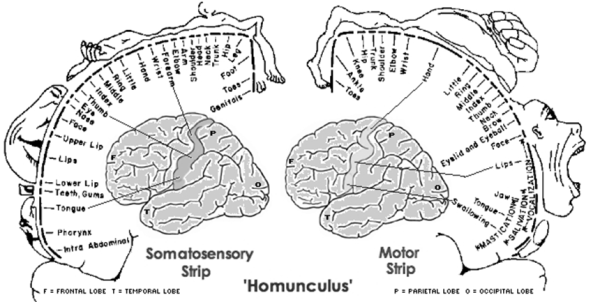
http://semestersequestered.wordpress.com/tag/cortical-homunculus/
Clinical Features
Haemorrhagic v infarct: Haemorrhage = sudden, headache, HTH, impair conscious state
Total ant circulation: hemiparesis/sensory, hemianopia, cortical signs
Partial ant circulation: 2/3 of above
Lacunar infarct: Any/ mixture of above without cortical signs
Post circulation syndrome: Brainstem/cerebellar features (diplopia, vertigo, dysphagia, ataxia, crossed motor/sensory & cranial nerve, crossed motor and ataxia, bilateral motor/sensory, hemianopia etc.)
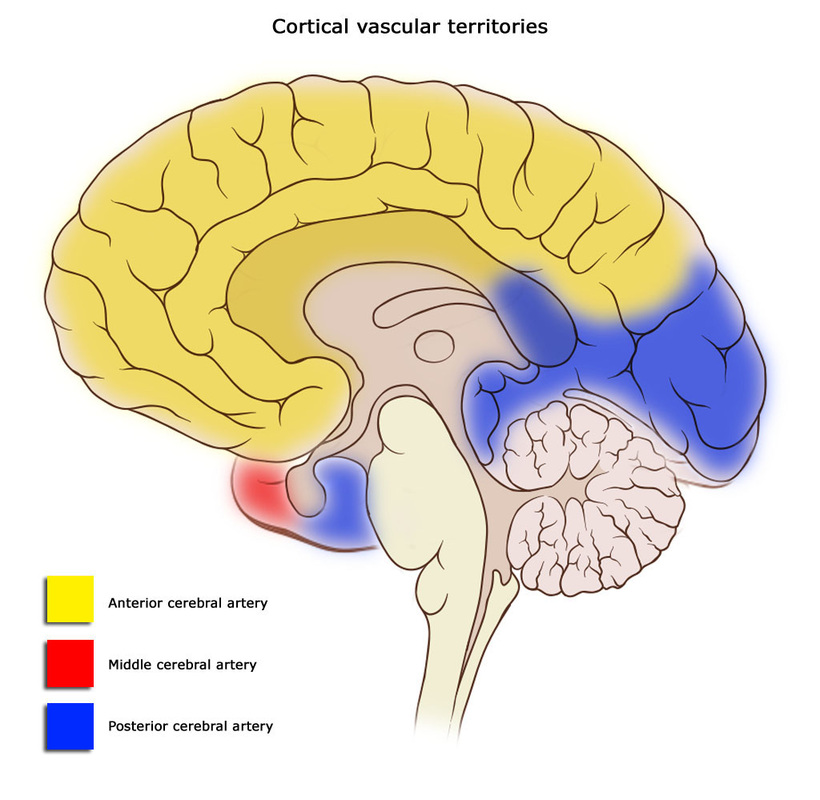
ACA:
A1 (circle of Willis):
A2:
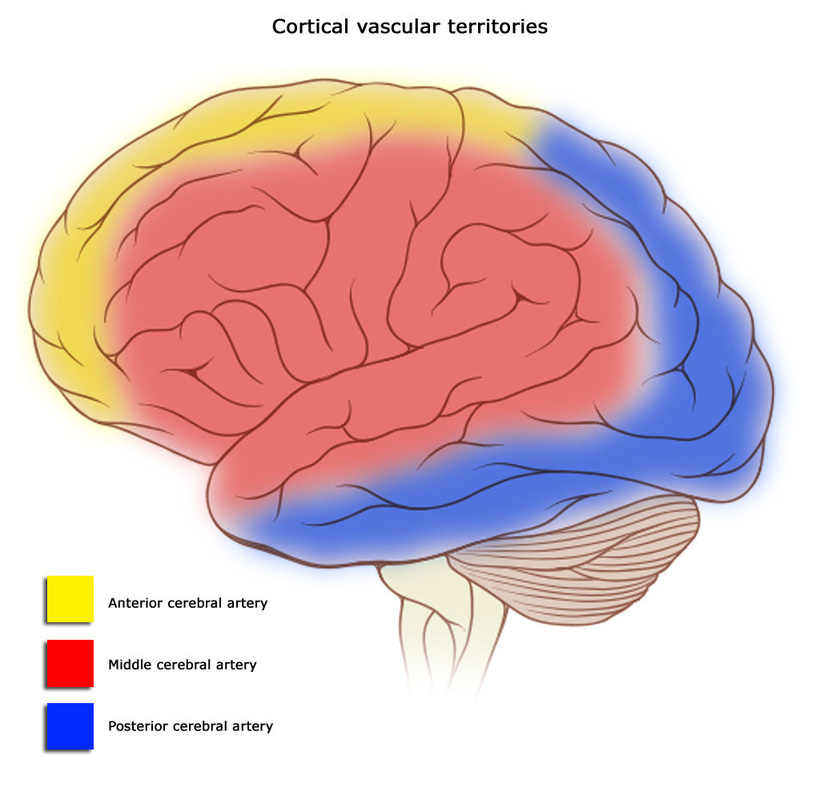
MCA (most common):
M1 (lenticulostriate):
Sup M2:
Inf M2:
Proximal occlusion
PCA:
P1 (circle of Willis):
P2:
Basilar a (locked in syndrome):
Pons (paramedian a):
Cerebellar peduncle (short circum)/ Cebellum (long circum):
PICA (Wallenberg/ lateral medullary):
Anterior spinal a (medial medullary):
Lacunar infarct (basal ganglia, thalamus, int capsule):
Anterior choroidal a:
TIA (<24h):
Investigations
URGENT: CT brain (Infarct may not appear until a few hours after stroke)
Bloods: FBC, UEC, Coags, BSL, lumbar puncture (SAH)
Bedside: ECG
Management
Risk Stratification after TIA: ABCD2 (0-7points)
Secondary prevention
Source
Dr David Dunbabin 2013
Toronto Notes 2012
Harrison's 16th ed
Haemorrhagic v infarct: Haemorrhage = sudden, headache, HTH, impair conscious state
Total ant circulation: hemiparesis/sensory, hemianopia, cortical signs
Partial ant circulation: 2/3 of above
Lacunar infarct: Any/ mixture of above without cortical signs
Post circulation syndrome: Brainstem/cerebellar features (diplopia, vertigo, dysphagia, ataxia, crossed motor/sensory & cranial nerve, crossed motor and ataxia, bilateral motor/sensory, hemianopia etc.)
ACA:
A1 (circle of Willis):
- IC- ant: C/L motor, sensory, hemianopia
A2:
- Motor/ sensory cortex: C/L leg motor and sensory loss
- 2o motor cortex: grasp/ suck reflex
- Corpus callosum: L "alien hand"
MCA (most common):
M1 (lenticulostriate):
- IC - post limb: C/L motor, sensory, hemianopia
Sup M2:
- Broca: Non-fluent aphasia (If dominant side), otherwise = neglect
- Motor/ Sensory cortex: C/L face + arm motor and sensory loss
Inf M2:
- Wernicke: Fluent aphasia (if dominant side), otherwise = neglect
- Optic radiation: C/L hemianopia
Proximal occlusion
- Above + I/L gaze preference
PCA:
P1 (circle of Willis):
- Midbrain: CN III, IV palsy
- Thalamus: sensory loss, amnesia, dec consciousness
P2:
- Medial cortical temporal/occipital
- C/L hemianopia/ quadrantanopia
- Left: Alexia (cannot recognise writing) without agraphia (cannot write)
- Left + Right: cortical blindness or prosopagnosia (cannot recognise faces)
Basilar a (locked in syndrome):
Pons (paramedian a):
- Quadriplegia/paresis
- A/dysarthria
- CN signs
Cerebellar peduncle (short circum)/ Cebellum (long circum):
- Impaired horizontal eye movements
- Cerebellar signs
PICA (Wallenberg/ lateral medullary):
- I/L: Horner's, facial sense, ataxia
- C/L: STT impairment (pain+temp) arms+legs
- Nystamus, vertigo, n+v
- Dysphagia, dysarthria, hiccups
Anterior spinal a (medial medullary):
- I/L: tongue weakness
- C/L: hemiparesis (facial sparing), impaired medial lemniscus (proprioception/ vibration)
Lacunar infarct (basal ganglia, thalamus, int capsule):
- Thalamus: C/L pure sensory loss
- IC: C/L sensory-motor loss, I/L: ataxia, leg paresis, dysarthria-clumsy hand syndrome
- NO CORTICAL SIGNS (eg. dysphasia, neglect, visual fields)
Anterior choroidal a:
- IC: C/L sensory-motor loss, I/L: ataxia, leg paresis, dysarthria-clumsy hand syndrome
TIA (<24h):
- Consciousness usually preserved; last for 5-15minutes
- Focal neuro deficits
Investigations
URGENT: CT brain (Infarct may not appear until a few hours after stroke)
Bloods: FBC, UEC, Coags, BSL, lumbar puncture (SAH)
Bedside: ECG
Management
- DRABCDE
- Ischaemic:
- Thrombolysis (rTPA)/ Aspirin/ Clopidogrel/ Heparin/ Warfarin
- Withhold antihypertensive unless >220/120 (ensure perfusion)
- Nil by mouth if dysphagia
- DVT prophylaxis
- Haemorrhagic:
- NO blood thinners!!
- Antihypertensives/ ICP lowering meds
- Rehab
Risk Stratification after TIA: ABCD2 (0-7points)
- Age - >60 = 1 pt
- BP - >140 Syst and/or >90 Diast = 1 pt
- Clinical Features – Unilat Weak = 2pt, Speech Disturbance = 1pt, Other = 0pt
- Duration - >/= 60 min = 2pt, 10-59 min = 1pt, <10 min = 0pt
- Diabetes – yes = 1pt, no = 0pt
- 4=2%, 5=16%, 6=36%
Secondary prevention
- Aspirin (Clopidogrel if C/I) --> no point combining
- Treat the cause
- If AF: CHADS2/ CHA2DS2VASc --> low risk (0) = Aspirin, high risk (2-6) = anti-coags
Source
Dr David Dunbabin 2013
Toronto Notes 2012
Harrison's 16th ed
