Acute Kidney Injury (AKI)
Definition
Characterised by:
Defined (any of the following):
Aetiology
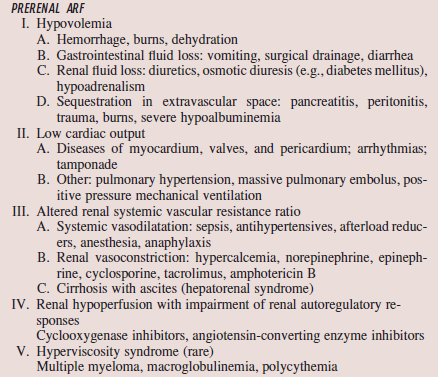
Pre-renal (~55%) = renal hypoperfusion
Clinical Features
Pre-renal
Renal
Post-renal
Investigations
Bedside: Urinalysis (blood/ protein = glomerular)
Bloods: FBC (eosinophil = alllergy), UEC, LDH (acute urate nephropathy/ tumour lysis syndrome), CMP (hyperphostataemia)
Imaging: US (calculi), CT KUB
Others: biopsy (when pre/post renal + ischaemic/nephrotoxic causes are excluded)
Complications
Management
Prevention!
Treatment
NOTE: No diuretics to prevent/ treat ARF, except in volume overload
Prognosis
50% mortality (dying from sequelae rather than ARF)
Details
Characterised by:
- Rapid (hours to days) decline of GFR
- Retention of nitrogenous waste products
- Abnormal ECF volume, electrolytes, acid-base balance
Defined (any of the following):
- Increase in SCr >/=0.3 mg/dL or 1.5x baseline in last 7/7
- Urine volume <0.5ml/kg/h for 6h
Aetiology
Pre-renal (~55%) = renal hypoperfusion
- Hypovolaemia
- Low cardiac output
- Altered systemic vascular resistance
- Drugs
- Hyperviscosity syndromes (rare)
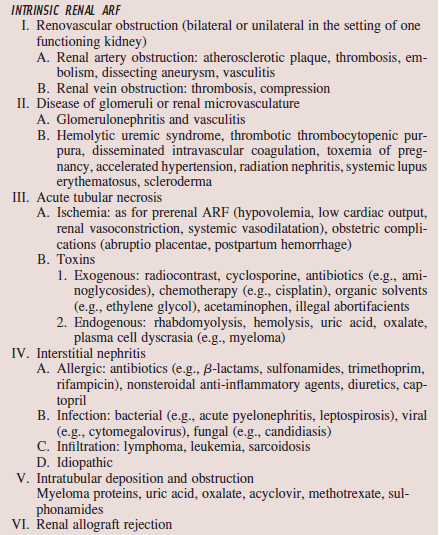
- Ischaemia and nephrotoxicity (~90%)
- Renal a/v obstruction
- Glomerular damage
- Tubulointerstitial damage
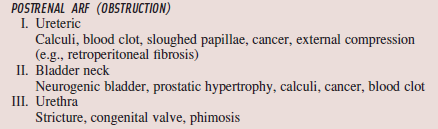
- Bladder neck obstruction (most common) = prostate pathology
- Calculi
Clinical Features
- Usually asymptomatic
- Oligouria (~50%)
Pre-renal
- Thirst
- Orthostatic dizziness
- ?Cardiac pathology
- ?Portal hypertension
Renal
- Flank pain (vessel occlusion)
- Hx of cardiac/ renal surg (cholesterol crystal emboli)
- HTN (malignant htn)
Post-renal
- Flank pain (renal collection sys distension)
- Suprapubic pain (bladder distension)
- Colicky flank pain (calculi/ prostatic disease)
- Neurgenic bladder
Investigations
Bedside: Urinalysis (blood/ protein = glomerular)
Bloods: FBC (eosinophil = alllergy), UEC, LDH (acute urate nephropathy/ tumour lysis syndrome), CMP (hyperphostataemia)
Imaging: US (calculi), CT KUB
Others: biopsy (when pre/post renal + ischaemic/nephrotoxic causes are excluded)
Complications
- inc ECF volume
- Hyperkalaemia
- Hyperphosphataemia
- Hypocalcaemia
- Anaemia (erythropoeisis)
Management
Prevention!
- Cardiovascular volume
- Adjust drug dosage
- IV saline -3/+6h from contrast (1-1.5ml/kg/h)
Treatment
- Treat the cause (vol/stop drug - pre; clear obstruction - post)
- Dialysis (see here for indications)
NOTE: No diuretics to prevent/ treat ARF, except in volume overload
Prognosis
50% mortality (dying from sequelae rather than ARF)
Details
- Hypoperfusion --> afferent (myogenic reflex + inc PGE2 production) + efferent ( Inc angiotensin II) --> afferent <-> + efferent >-< --> intraglomerular pressure preserved
- If MAP <~80mmHg, autoregulation fails --> GFR dec
- Tubular epithelium most sensitive to ischaemia
- Tubuloglomerular feedback: inc salt in distal tubule --> epithelium (macular densa) sense --> juxtaglomerular cells (smooth m cells) --> constrict afferent arteriole/ deactivate renin production --> dec blood flow
|
|
|
Source
Harrison's 16th Ed
Harrison's 16th Ed
